 Where We Work
Where We Work  Press Room
Press Room  FACT Project
FACT Project  Passages Project
Passages Project  Learning Collaborative
Learning Collaborative  Search All Resources
Search All Resources  Social Norms
Social Norms  Fertility Awareness Methods
Fertility Awareness Methods Is a health systems strengthening approach enough? Assessing USAID’s family planning contributions in Jordan
The US government invested over $50 billion in global health over the last five years. Last year specifically, USAID laid out its first ever Vision for Health Systems Strengthening, defining health systems strengthening (HSS) as a capacity building approach that supports quality service provision, extends the coverage of care, and provides financial protections, all while improving the responsiveness and resilience of local health institutions. The Vision’s purpose is to renew its commitment to HSS and provide a strategic framework for implementation, but HSS can be a huge undertaking for local governments and health institutions. We know that HSS investments matter, but in what contexts does HSS programming work best in improving family planning outcomes?
HSS in Jordan: Setting the stage
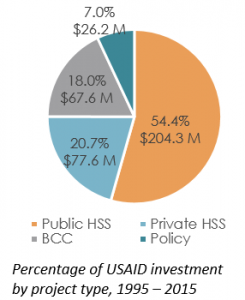 We can learn a lot from USAID’s family planning investments in Jordan. Jordan’s national family planning goal is to reach a replacement level of fertility of 2.1 by 2030 in order to ease the pressures of massive population growth, refugee influxes, and scarce natural resources. For over a decade, the total fertility rate (TFR) in Jordan has stagnated. Contraceptive prevalence is high, but less-effective, traditional methods have been on the rise, comprising one third of the method mix in 2012. USAID has invested close to $445 million in Jordan’s health sector, with approximately 75% targeting HSS in maternal and child health and reproductive health. As part of an assessment of USAID’s family planning program in Jordan over the last decade, we systematically reviewed existing program documentation and conducted interviews with key stakeholders. These documents guided a set of recommendations provided to the USAID/Jordan mission for future family planning investments.
We can learn a lot from USAID’s family planning investments in Jordan. Jordan’s national family planning goal is to reach a replacement level of fertility of 2.1 by 2030 in order to ease the pressures of massive population growth, refugee influxes, and scarce natural resources. For over a decade, the total fertility rate (TFR) in Jordan has stagnated. Contraceptive prevalence is high, but less-effective, traditional methods have been on the rise, comprising one third of the method mix in 2012. USAID has invested close to $445 million in Jordan’s health sector, with approximately 75% targeting HSS in maternal and child health and reproductive health. As part of an assessment of USAID’s family planning program in Jordan over the last decade, we systematically reviewed existing program documentation and conducted interviews with key stakeholders. These documents guided a set of recommendations provided to the USAID/Jordan mission for future family planning investments.
The effect of USAID programming on Jordan’s family planning outcomes
Existing documentation showed output-level improvements in the quality of services and access to reproductive health and maternal, newborn, and child health services over the last decade. The list of milestones is lengthy, but some key examples from our assessment report include:
- Establishing 21 Comprehensive Post-Partum centers
- Renovating and equipping 25 public hospital departments and 318 primary health care centers
- Conducting 1.4 million family planning counselling visits, and generating 90,000 new clients of modern family planning methods
- Training 6,000 public health service providers and establishing quality assurance teams at 200 centers
- Training 1,500 pharmacists and 900 physicians in the private sector on family planning services and counselling
- Establishing 106 community health committees linked to primary healthcare centers
- Securing an improved logistics systems for contraceptives, which was assumed by Jordan’s Ministry of Health in 1999 to manage contraceptive distribution
- Introducing standards of care for health centers, improving supervision, clinical guidelines, and information systems
Yet despite these successful outputs, Jordan’s total fertility rate and modern contraceptive prevalence rate (mCPRT) lagged during the same time period.

Emergency neonatal care unit in Jordanian public hospital funded by USAID
Why weren’t HSS inputs more effective for family planning outcomes?
There are two explanations for the weaker HSS effect on fertility stagnation in Jordan. First, focusing on HSS programming increased the number of outlets for services, but could not address socio-normative barriers to family planning. As discussed in the second post of this series, indirect determinants of fertility—such as social norms around family size and son preference—play a powerful role in family planning decision-making in Jordan. These cannot be tackled alone with an HSS approach. Second, heavy HSS investment may have inadvertently decreased Jordan’s political and economic ownership over its reproductive health programs. Evidence suggests three types of government commitment (expressed, institutional, and financial) are needed to enable a supportive environment for family planning programs. Field interviews repeatedly confirmed the existence of “verbal” commitment by senior government and central ministry of health staff for family planning programs, but limited institutional and financial commitment. This is consistent with desk review findings, which highlighted the lack of government funding as the key limiting factor in family planning program sustainability. This suggests that a lot more needs to be done to ensure that HSS programs achieve programmatic sustainability.
Moving forward with a balanced approach
Relative to other behavior change and advocacy investments, USAID’s HSS-dominant portfolio – which aimed to improve maternal and child health and reproductive health services more broadly – may have limited impact on family planning outcomes. Using EngenderHealth’s Supply-Enabling Environment Demand (SEED) Model, we apply a framework for family planning programmatic and policy decision-making to the USAID/Jordan portfolio:
|
SEED Model Component |
Application: USAID/Jordan Portfolio |
| Attend the availability and quality of services and other supply-related issues |
|
| Strengthen health systems and foster an enabling environment for SRH-seeking behavior |
|
| Improve knowledge of SRH and cultivate demand for services |
|
Examining more than a decade of programmatic implementation stakeholders in Jordan provides an opportunity to suggest future programming priorities for similar contexts. In countries with relatively high access to, and use of, family planning services, an exclusively HSS approach may not be the best investment to affect TFR and CPR stagnation. More comprehensive programmatic activities that address community and familial fertility norms, increase options available to couples, and support providers will evolve the landscape of reproductive health service delivery, and enable countries like Jordan to meet their fertility goals.